
8
Chapter Objectives
- Describe the anatomical variation, population incidence of a range of phenotypes, and Australian and New Zealand context of select examples of the respiratory system, including the:
- lung fissures
- Discuss the clinical and/or professional impact of anatomical variation of the respiratory system on patients and/or professional settings
Lung Fissures
Variation Classification: Morphology and Frequency
Description of Anatomy
The lobes of the lung are separated by visceral pleura lined grooves referred to as lung fissures. The right lung typically has two fissures: the oblique fissure separating the superior and middle lobes from the inferior lobe; and the horizontal fissure separating the superior and middle lobes of the right lung. The left lung typically has one fissure: the oblique fissure separating the superior and inferior lobes of the left lung. The fissures exhibit morphological variation in their depth and completeness ie. whether it completely separates the two lobes that it lies between. We can also observe frequency variation in the absence of fissures and accessory fissures in some cases. Accessory fissures are fissures additional to the oblique and horizontal fissures described above and can occur in both the right and left lungs.
Test your knowledge of the anatomy of the lung by identifying each of the lobes and fissures of the right lung in the below diagram. Check each of your answers by clicking on the question mark icon.
[Image: L. Gregory CC BY-NC 4.0]
Examples of Phenotypic Variation
Morphological variation: Lung fissures can be classified into two phenotypes based on their depth (shallow or deep) and two phenotypes based on completeness (complete or incomplete). Deep fissures are defined as those fissures that extend to the hilum of the lung, with complete separation of the lobes with visceral pleura. Incomplete fissures are shortened fissures that do not extend the full distance of the complete fissure and do not completely separate the adjacent lung lobes.
Frequency variation: In some cases fissures can be absent such as the horizontal fissure of the right lung. Accessory fissures can also present due to additional folds in the visceral pleura and/or a lack of fusion of bronchopulmonary segments during development. They are named according to their respective lobe and approximate location they are located in such as a superior accessory fissure of the inferior lobe. In most cases these accessory fissures are incomplete and do not extend the full distance of the lung tissue to completely separate adjacent lobes.
The number of lobes of the lung is directly correlated with the number of secondary/lobar bronchi in the body with each lobe having one lobar bronchus which is accompanied with blood vessels, lymphatics and nerves. The presence of shallow or incomplete fissures does not typically impact the branching pattern of these lobar bronchi. It is possible however that absent fissures may have underlying differences in bronchial patterns due to altered embryological development.
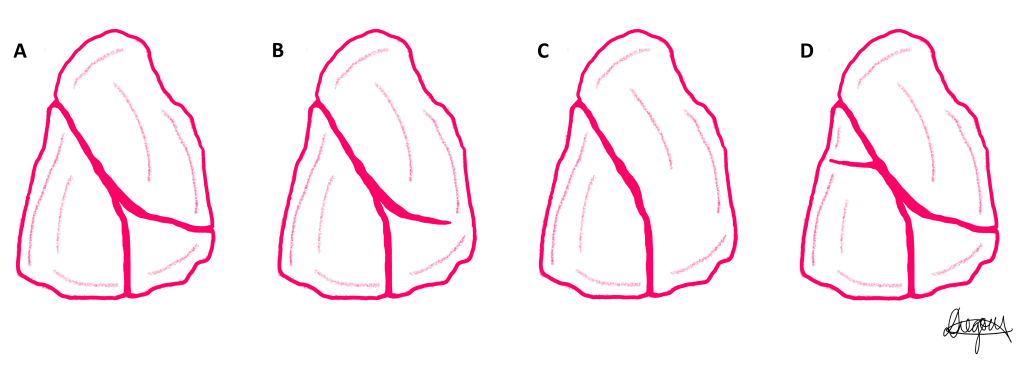
Four phenotypes of the lung fissures of the right lung demonstrating variation of completeness and frequency are presented in a series of diagrams below. Use the slider tool to move between each phenotype and read the text underneath that describes each phenotype. By dragging the slider tool you can view the transition between each phenotype to clearly see how each phenotype differs from the next.
The same four phenotypes of the lung fissures are presented in a single diagram below.
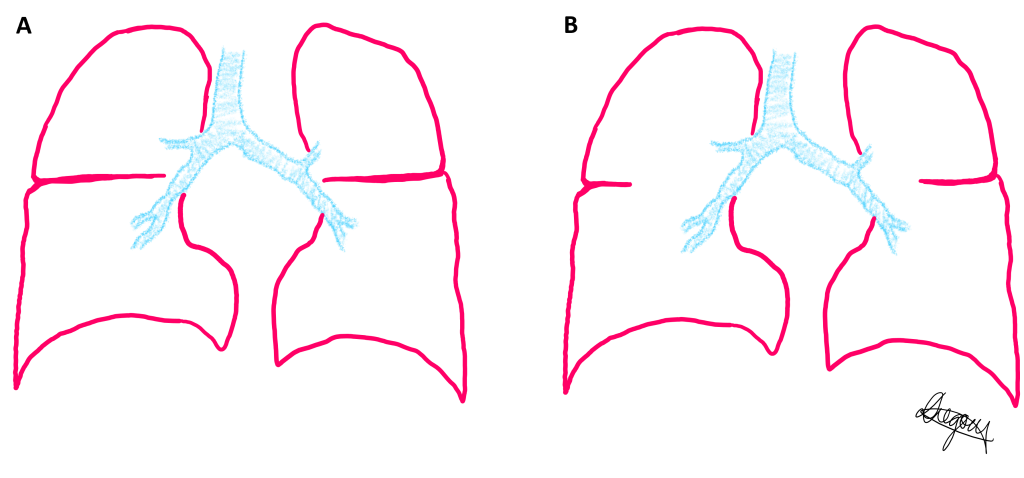
Two phenotypes of the depth of the lung fissures are presented in a series of diagrams below of the right and left lung in a coronal slice. Use the slider tool to move between each phenotype and read the text underneath that describes each phenotype. By dragging the slider tool you can view the transition between each phenotype to clearly see how each phenotype differs from the next.
The same two phenotypes of the depth of the lung fissures are presented in a single diagram below.
Population Frequencies of Phenotypic Variation
| Source | Phillips et al. (2020) | Mote et al. (2018) | Nene et al. (2011) | Meenashi et al. (2004) | Sudikshya et al. (2018) | George et al. (2014) | Unver Dogan et al. (2015) |
| Population | Australian | Indian | Indian | Indian | Nepalese | Indian | Turkey |
| Source material | CTa scans | Donor lungs | Donor lungs | Donor lungs | Donor lungs | Donor lungs | Donor lungs |
| n (patients) | 86 | 30 | 50 | 30 | 50 | 65 | 210 |
| Right Horizontal Fissure | |||||||
| Complete | 88.4% | 43.3% | 78% | 20.1% | 52.18% | 41.55% | 87.62% |
| Incompleteb | 9.3% | 43.7% | 8% | 63.3% | 34.78% | 35.38% | 8.57% |
| Absent | 2.3% | 13.3% | 14% | 16.6% | 13.04% | 23.07% | 3.81% |
| Right Oblique Fissure | |||||||
| Complete | 95.3% | 76.7% | 92% | 63.4% | 69.57% | 96.93% | 98.1% |
| Incomplete | 3.5% | 23.3% | 6% | 36.6% | 30.43% | 3.07% | 1.43% |
| Absent | 1.2% | 0 | 2% | 0 | 0 | 0 | 0.48% |
| Left Oblique Fissure | |||||||
| Complete | 95.3% | 83% | 88% | 54.4% | 48.15% | 84.94% | 99.05% |
| Incomplete | 3.5% | 17% | 12% | 46.6% | 51.85% | 15.06% | 0.95% |
| Absent | 1.2% | 0 | 0 | 0 | 0 | 0 | 0 |
| Right Accessory Fissures | |||||||
| Complete
Incomplete |
5.8%
3.5% |
0
0 |
2%
16% |
3.3%* | 30.43%* | 4.61%* | 0.48%
4.76% |
| Left Accessory Fissures | |||||||
| Complete | 0 | 0 | – | 10%* | 33.33%* | 2.73%* | 2.38% |
| Incomplete | 2.3% | 0 | 50% | 1.43% | |||
a computed tomography, b incomplete = stage 2 and stage 3 combined, *accessory fissures were not classified on completeness in these studies. Bold indicates majority.
Australian and New Zealand Context
Phillips et al. (2020) investigated the incidence of accessory fissures and the percentage of fissures complete in a paediatric Queensland Australian population. The authors noted that the right horizontal fissure, right oblique fissure and left oblique fissure were absent in 2.3%, 1.2% and 1.2% of the population. Accessory fissures were more frequent in the right lung (9.3%) compared to the left lung (2.3%), and more frequently located in the inferior lobe. Incomplete fissures were more common in the horizontal fissure of the right lung (9.3%) compared to the oblique fissures of the right (3.5%) and left (3.5%) lungs. Fifty percent of accessory fissures were of the incomplete phenotype (Phillips et al., 2020). The depth of the fissure was not quantified in this study.
Case Study on Lung Fissures: Case of Pneumonia
A 84 year old female patient born in Australia presents with a Streptococcus pneumoniae infection in the right lung. The radiology report indicates that the infection is currently localised in the middle lobe. Use the image slider to compare the radiograph of the patient before treatment (left image) with radiopaque (white) consolidation in the right cardiophrenic angle (between the cardiac shadow and right dome of the thoracic diaphragm) with the radiograph of the same patient 10 days of treatment (right image) with now a radiolucent (black) right cardiophrenic angle.
Figure 8.3:Thoracic radiographs in a posteroanterior projection [Case courtesy of Mohammad Osama Hussein Yonso. Radiopedia.org, rID: 87716CC-BY-SA 3.0]
Pneumonia is an infection of the lungs caused by bacteria, viruses or fungi. The small alveoli become filled with fluid preventing gas exchange from occurring. The streptococcus pneumoniae bacterium enters the oral or nasal cavity typically from close contact with another person through respiratory droplets. It is in the nasopharynx that the bacteria colonises first and can spread to the paranasal sinuses, middle ear or lower respiratory tract.
QUESTION 1: Draw a flowchart of the passageway of the Streptococcus pneumoniae from the nasopharynx to the middle lobe of the right lung by naming each anatomical structure it passes through.
QUESTION 2: Once colonised in the middle lobe of the right lung, what prevents the bacteria from spreading to the other lobes of the right lung?
- Refer to the population frequencies of phenotypic variation table above: What is the likelihood that the patient has an incomplete horizontal fissure?
- Consider the consequences if the patient had an incomplete or absent horizontal fissure
- Would the depth of the oblique and horizontal fissures affect the patient’s case?
References and Further Reading
George, B.M., S.B. Nayak, and S. Marpalli, Morphological variations of the lungs: a study conducted on Indian cadavers. Anat Cell Biol, 2014. 47(4): p. 253-258.
Meenakshi, S., K.Y. Manjunath, and V. Balasubramanyam, Morphological variations of the lung fissures and lobes. Indian J Chest Dis Allied Sci, 2004. 46(3): p. 179-82.
Mote, D., P. Awari, and V. Bharambe, A study of fissures and lobes of lungs from clinical perspective. Pulsus J Surg Res, 2018. 2(2): p. 41-43.
Nene, A.R., K.S. Gajendra, and M.V.R. Sarma, Lung lobes and fissures: a morphological study. Anatomy, 2011. 5(1): p. 30-38.
Phillips, R., Reynolds, M.S., and Gregory, L.S. (2020) Anatomical variation of the fissures of the lungs in an Australian population using computed tomography. (Bachelor of Biomedical Science (Honours) thesis, Queensland University of Technology; data not yet published).
Sudikshya, K., et al., Variations in human pulmonary fissures and lobes: a study conducted in nepalese cadavers. Anatomy & cell biology, 2018. 51(2): p. 85-92.
Unver Dogan, N., et al., Major anatomic variations of pulmonary fissures and lobes on postmortem examination. Acta clinica Croatica, 2015. 54(2): p. 201-207.
